Hair Loss
links: reference: Saving my progress: https://raypeatforum.com/community/threads/hair-loss-thinktank-passionate-and-or-intellectual-people.40689/page-4 - https://raypeatforum.com/community/threads/hair-loss-thinktank-passionate-and-or-intellectual-people.40689/post-649987
- https://www.youtube.com/watch?v=mMgN6hYQgZ8 To read: https://raypeatforum.com/community/threads/anyone-here-stopped-their-hairloss.19225/
- Random oils
- If Calcification Is The Root Of Hair Loss - How To Reverse It? (Magnesium , D, A, K2, Potassium)
- (Taylor, 2008) Big head? Bald head! Skull expansion: alternative model for the primary mechanism of AGA
- https://raypeatforum.com/community/threads/capilia-longa-for-hair-growth-derived-from-turmeric.25450/
- https://raypeatforum.com/community/threads/its-not-dht-its-a-metabolite-for-mpb.26672/
- Topical Pirfenidone - The real answer to inflammation and fibrosis …
- https://raypeatforum.com/community/threads/is-hairloss-mainly-a-growth-hormone-issue.40661/
- https://raypeatforum.com/community/threads/scalp-progesterone-for-hair-loss-experiment.5833/ - 89 page megathread
- https://folliclethought.com/updates/
- https://raypeatforum.com/community/threads/why-i-regret-giving-hair-loss-advice-and-a-major-breakthrough.19046/ Sebum 5-12-2021
Hair Loss #
“The hair follicle itself is a complicated mini-organ that stands to be negatively affected by even subtle shifts in the efficiency with which energy is generated. In fact, because of the already inherent inefficiency of metabolism present therein, the hair follicle is one of the most sensitive among all the organs to these shifts.”
-
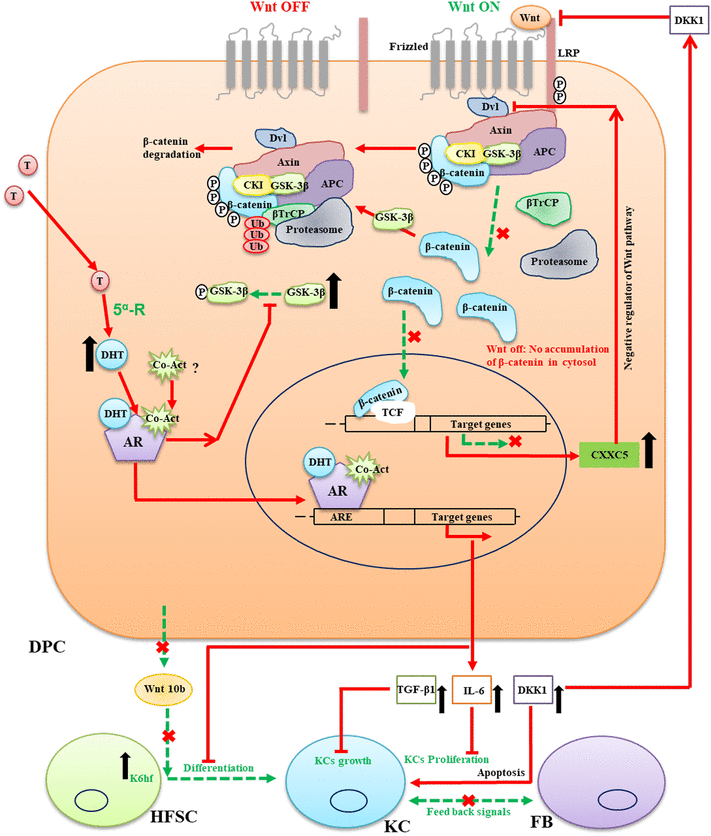
- DPC = dermal papilla; HFSC = hair follicle stem cell
-
- Apparently hair anywhere besides the legs is estrogen driven - estrogen irritating the adrenals leading to higher peripheral DHEA->androgens leading to hair growth.
- Hamilton’s castrates/psuedohermaphrodites had reduced oily secretions from sebaceous glands and minimal to no dandruff.
- Associated with arterial stiffness and metabolic resistance. Risk for hyperinsulinaemia and cardiovascular disease.
- In cases of MPB, there can be up to 4x normal amounts of Mast Cell in the scalp.
- Sebaceous cell hyperplasia
-
Thematic review series: skin lipids. Sebaceous gland lipids: friend or foe?
- They claim that respectively low/high Wnt/c-Myc/Hedgehog leads to hair follicle vs sebaceous gland differentiation from epithelial progenitor cells:
- Mice with mutations in β-catenin, which decrease Wnt signaling through a binding defect in β-catenin, have an increased number of sebaceous glands over normal mice (sounds like the opposite of the above claim)
- c-Myc is downstream of β-catenin and overexpression = increase in sebaceous gland size/number (proliferation) and decrease in number of hair follicles.
- They claim that respectively low/high Wnt/c-Myc/Hedgehog leads to hair follicle vs sebaceous gland differentiation from epithelial progenitor cells:
-
Thematic review series: skin lipids. Sebaceous gland lipids: friend or foe?
- Nizoral is pretty meh compared to purer ketoconazole products. Racosinate = carcinogenic; sulfate = irritation, etc.; benzyl alcohol = dryness. It’s also kind of just a meme considering the short time frame is spends on your scalp
Anatomy #
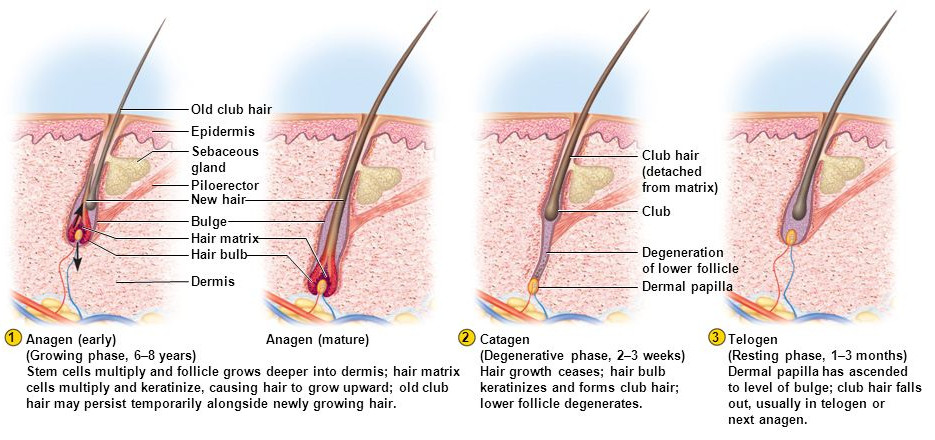 The red tissue holding it is the arrector pili muscle, which conencts the dermal surface and the follicle and contraction (piloerection) causes goose bumps.
The red tissue holding it is the arrector pili muscle, which conencts the dermal surface and the follicle and contraction (piloerection) causes goose bumps.
- Fibroblasts tell keratinocytes when to divide and induce repeated growth and are a signaling center for follicular stem cells, which decline with age, thus reducing the number of fibroblasts.
Growth Cycle #
-
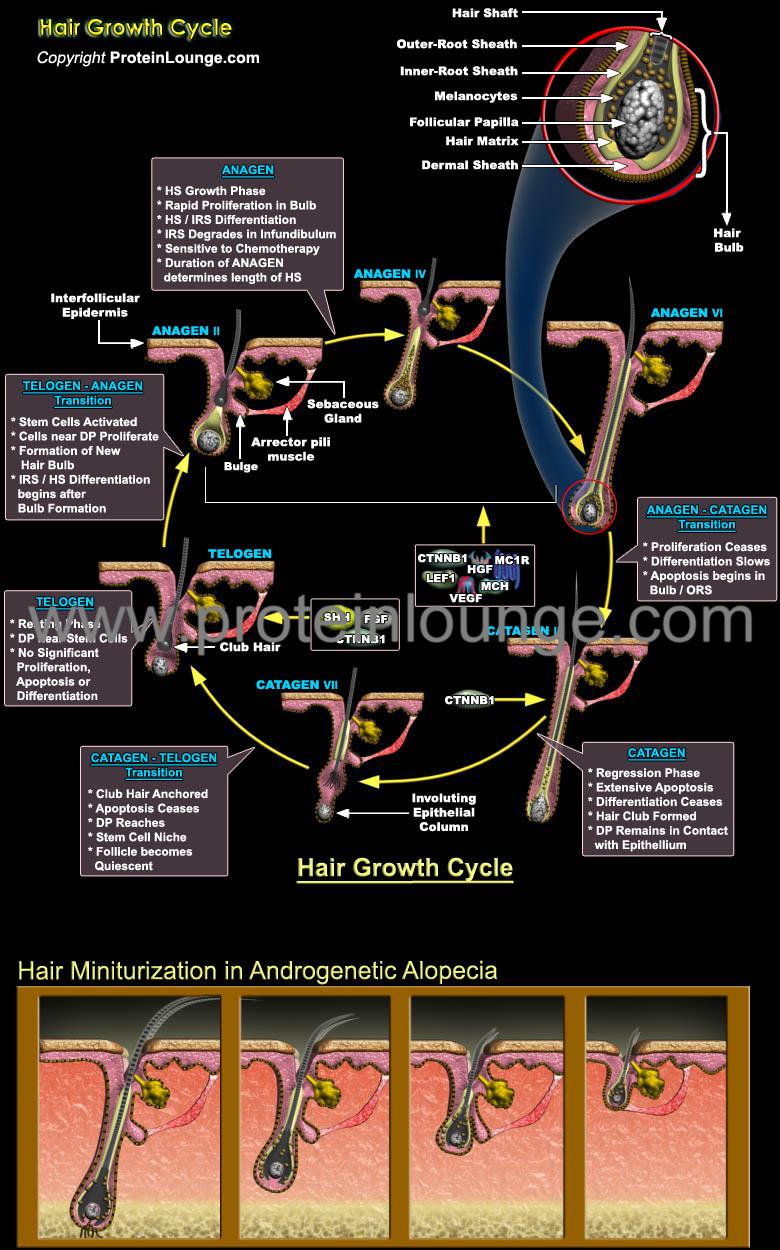
-
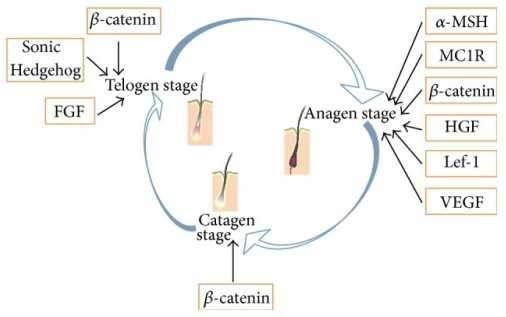
- TGF-β plays a key role in the catagen phase. Inhibitor of keratinocyte proliferation and inductor of keratinocyte apoptosis R
- IGF-1 inhibits the catagen and telogen phases, favoring anagen.
-
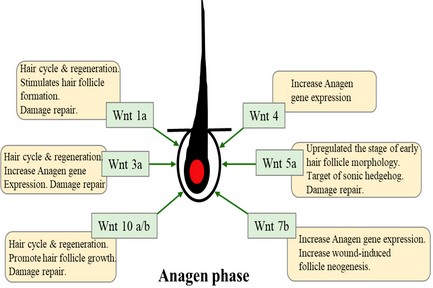
- Targeting Wnt/β-Catenin Pathway for Developing Therapies for Hair Loss (Choi 2020)
- Also implicated is TGF-β + BMP (Bone morphogenic protein)
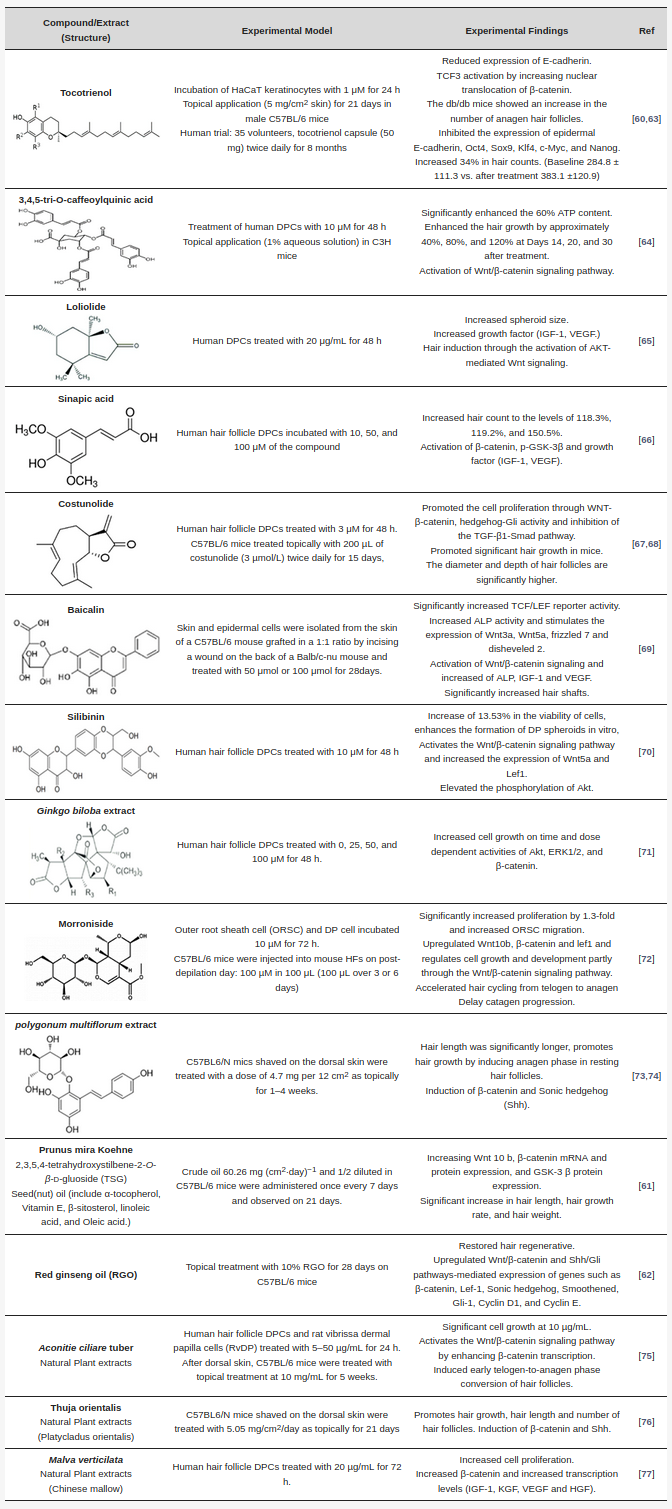
- The Molecular Mechanism of Natural Products Activating Wnt/β-Catenin Signaling Pathway for Improving Hair Loss (Shin 2022) has 3 more big lists with some overlap to above.
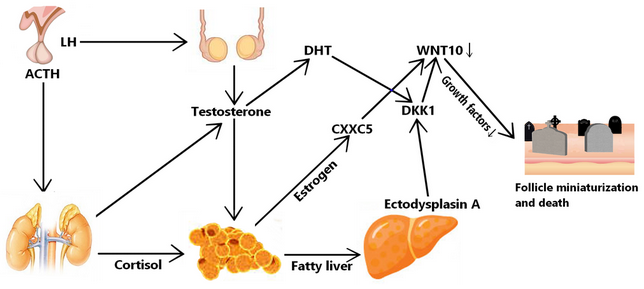
Hormonal Profile #
-
This study adds evidence to the possibility that hyperadrenalism may be an important element in the complex biochemistry of male pattern baldness. R
- The biochemistry of androgens, particularly DHEA-S, suggests that adrenal hyperactivity (i.e., low thyroid) may initiate alopecia in young men who are generally susceptible. R
-
https://raypeatforum.com/community/threads/the-hormonal-profile-of-mpb.40652/#post-647488
- Significantly elevated Androstenedione, Luteinizing Hormone, Estradiol, and Cortisol.
- Moderately elevated DHEA-S, free Testosterone, Progesterone, Prolactin, and testosterone.
- Significantly decreased FSH and SHBG
-
Also correlated with lowered Aldosterone, Parathyroid Hormone, FAI, and insulin resistance. (FAI = free androgen index, a ratio used to determine abnormal androgen status.) (100 * Test./SHBG)
-
Higher levels of Aromatase where there’s still hair R
- Aromatase can be increased locally with dexamtheasone or glucorticoids. It’ll thin the skin.
Prolactin #
- Apparently Pituitary Gland prolactin suppression causes autocrine prolactin to increase, which is how Cabergoline can cause hair loss.
DHT #
Treatment #
- Something to know wrt. physiology of topicals: compounds remain in the dermis at 4mm just before vascularization.
- Rosemary and mint essential oil might help with hair growth?
- TWIST1 inhibitors like ADQ.
- Centele Asiatica - upregulates VEGF. Esoteric though; idk its effects on 5-AR
- Topical cyclosporine
- HIF-1α is a potential treatment:
- Insights into male androgenetic alopecia using comparative transcriptome profiling: hypoxia-inducible factor-1 and Wnt/β-catenin signalling pathways
- Hypoxia inducible factor-1α promotes trichogenic gene expression in human dermal papilla cells
- HIF-1α Stimulators Function Equally to Leading Hair Loss Agents in Enhancing Dermal Papilla Growth
- Prolactin antibodies
- Sirsad thinks/thought that this was the most promising treatment yet
Protocol #
- My kitchen sink topical would be something like a water-soluble bottle and another lipid-soluble bottle of the following:
- 0.2% caffeine
- Melatonin
- DKK inhibitors: Niacinamide, threonic acid
- Basically everything in the placode serum besides the acrylates/polymers
- WNT/β-catenin inducers:
- Those mentioned in Choi et al above (Ginseng, caffeoyl compounds, and the other weird stuff)
- Redensyl
- TWIST inhibitors:
- Bioenergetics: Solban, Caffeoylquinic Acid (again)
- PGE2 inducers like castor oil? Salicylic acid might remove this from the picture though.
- Phytoceramides/phyto stem cells?
- SkQ1?
- Sirsadalot vouches carnosic acid (in PEG400, got up to 100mg/mL) + idebenone for preventing dandruff (put it in head and shouylders)
- Progesterone for paracrine prolactin inhibition? Could be risky.
-
Bryan Johnson’s NEW protocol: #
- Bryan Johnson’s OLD
Protocol 1mL applied daily
- Caffeine USP 1%
- Finasteride USP 0.25% (thus 2.5mg. In reality 0.2 (0.25% 100μl, or 0.025% 1 mL) is an ideal low range if I were to try this)
- Minoxidil USP 5% (I go over this there kinda)
- Azelaic Acid 1.5%
- The efficacy and safety of minoxidil 5% combination with azelaic acid 1/5% and caffeine 1% solution on male pattern hair loss this paper is literally unobtanium
- Diclofenac 0.5%
- COX-2 inhibitor.
- Holy shit, all NSAIDs are SULT inhibitors.
- Tea Tree Oil 5%
- Rosemary Oil 0.37% (so 3.7mg)
- Ginko Biloba 0.05%
- Biotin 0.01%
- Melatonin USP 0.0033%
- All dissolved in Trichosol, which is a hydrophillic solution thing. The carrier is honestly very important, or else there may not be a lot stopping it from going systemic
- Other pharmeceutical preparations of minoxidil and such around the world use this as a solvent as well. So if I wanted to get my hands on this stuff I’d probably look for a minox product. Supposedly not the best for post-application look compared to foam>hydroalcoholic as a close second.
- He also does + PRP, dutasteride mesotherapy, autologous exosomes, laser cap
- Throw in Carnosic Acid (which I just realized is the primary component of rosemary) and the other stuff in Neotopical
Novel Chemicals #
- https://thekaneshop.com/product-category/on-sale/ a lot of them can be bought here.
- https://www.hairlosstalk.com/interact/forums/new-research-studies-and-technologies.24/
- https://www.hairlosstalk.com/pipeline/
- miR-205 for unstiffening follicle stem cells.
- SM04554, another WNT activator, I think. Induces follicular neogenesis, regrowing dead hair. It’s in phase 3 clinical trials.
- Clascoterone: topical Androgen Receptor antagonist that has minimal systemic absorption. Went through phase 3. Not sure how efficacious it is.
- SCUBE3: Sonic Hedgehog activating peptide. It’s a long ways away.
- Is it all sunshine and roses if it goes systemic?
- This mechanism previously posed a risk for skin cancer or something >10 years ago—but SCUBE3 does not have this.
- Coordinated hedgehog signaling induces new hair follicles in adult skin
- Hedgehog signaling reprograms hair follicle niche fibroblasts to a hyper-activated state
- https://www.hairlosscure2020.com/the-sonic-hedgehog-pathway-an-unrealized-dream/
- Plenty of coverage on youtube.
- In an interview with Makism Plikus who made it, he said the new growth might not necessarily look like the hair on your head, due to the nature of the growth…? Worrying.
- Is it all sunshine and roses if it goes systemic?
- Pyrilutamide
- GT20029
- TDM105795
- Clascoterone (CB-03-01) (Breezula) readily available. Topical AR antagonist. Why instead of RU, I dunno. First FDA-appoved anti-androgen in 2026 and was approved in 2020 for Acne, under the name Winlevi.
- Can shut down the adrenal axis
- Stuff from the Cure Protocol for wound-induced hair neogenesis:
- GNE-7883 (Pan-TEAD antagonist)
- Vemurifenib (BRAF inhibitor)
- CHIR99021 (GSK-3β inhibitor)
- WAY-316606 0.5% (SFRP1 inhibitor)
- WAY-262611 (Dkk1 antagonist)
- TDM-105795 (Thyroid receptor agonist)
- JXL-069 (MPC inhibitor)
- Minox (Potassium channel opener)
- Decitabine (DNMT inhibitor)
- Imiquimod (TRPA1 agonist)
- Stuff from the Cure Protocol for hair follicle miniaturization:
- TM-5614, a PAI-1 inhibitor (plasminogen activator inhibitor-1). Sold on Umbrella.
- I think it might be related to prolactin?
- Abiraterone Acetate (17α-Hydroxylase inhibitor, just like ketoconazole)
- Harmine 19a (cope?) (TWIST1 inhibitor)
- BIM I (PKCα inhibitor)
- Sapanisertib (Pan-mTOR inhibitor)
- FK506 (BMP pathway promoter)
- Y-39983 (ROCK inhibitor)
- SIS3 16d (Smad3 inhibitor)
- TM-5614, a PAI-1 inhibitor (plasminogen activator inhibitor-1). Sold on Umbrella.
- Fluridil (topilutamide)
Microneedling #
- 1200-1600 needle strikes per cm². 1mm, however 1.5mm dermaroller is fair since it doesn’t penetrate as deeply as the motorized devices. Once every week, maybe once every 2 weeks.
- Either wait a few hours after minox to microneedle (bad idea if you’re using peppermint oil, and so I assume rosemary as well.)
- … or you can apply all your topicals the morning after (probably the better option if you’re using topical dut because fuck that, but if weekly I’d microneedle the night after weekly dut day)
- … or just skip a minox(+dut) dose and only do minox 6 days a week. So like dut on sunday and microneedle on monday night or something.
Peptides/Serums #
I actually ought to look up clinical trials for some of these formulations like Redensyl, because they may be legit for regrowth
-
RevivserumsThis (discontinued!) peptide hair serum has:
- Oligopeptide-54: promotes growth & revitalization of follicles and circulation
- Decapeptide-10: a DKK-1 inhibitor
- Decapeptide-18: similar to WNT10
- Additionally contains niacinamide, caffeine, B5, and PEG 20/23 dimethicone, acrylate crosspolymer, sodium acrylaates copolymer & lecithin, triethanolamine, fragrance.
- They have dozens of formulations for various skin, hair, and nails conditions.
-
This is the new one, the hair stimulating serum, which has:
- 5.0%
Redensyl (this paper goes very in-depth)
- Contains dihydroquercetin-glucoside (DHQG). Polyphenol which stabilizes fibrillar collagen forms and inhibits melanogenesis. Activates follicle stem cell division, activates Bcl-2 (inhibits apoptosis) and WNT
- Also an agonist of AdipoR2 and opioid receptors.
- EGCG2: General antioxidant and cytokine reducer
- Glycine, zinc chloride, meta-bisulfite, glycerin.
- Do not store at temperatures over 10°C?? (50°F)
- Contains dihydroquercetin-glucoside (DHQG). Polyphenol which stabilizes fibrillar collagen forms and inhibits melanogenesis. Activates follicle stem cell division, activates Bcl-2 (inhibits apoptosis) and WNT
- 1.50% Capixy®
- Acetyl tetrapeptide-3 (probably safe) mixed with red clover extract, which is rich in biochanin A, a 5-ARi.
- 3.0% Procapil®
- Consists of Biotinyl-GHK, apigenin, oleanolic acid (a 5-ARi).
- Keratinocyte growth factor
- Myristoyl pentapeptide-17 (keratin stimulating)
- GHK
- And mothafuckin’ phyto stem cells: PhytoCellTec Malus Domestica, PhytoCellTec Argan, Celtosome Crithmum Maritum, Anasensyl
- Caffeine, soy isoflavones, grape seed proanthocyanidins, horse chestnut
- Nettle root and saw palmetto. GOT EM!
- 5.0%
Redensyl (this paper goes very in-depth)
- Stemoxidine (Diethyl Lutidinate; Mexoryl) patented by L’Oreal in 2012. P4H inhibitor; induces hypoxia in stem cells, raising oxygen levels at the layer near the skin surface, lengthening the kenogen phase.
- Sepicontrol A5: 5AR inhibitor.
Hair Transplant #
- 2023-10-31
- Don’t cheap out on the surgeon, since apparently there’s quite a bit you can get wrong? Like angulation of the grafts, for one thing.
- Dr. Laorwong/Absolute might be the best clinic? https://looksmax.org/threads/give-your-opinion-on-this-hair-transplant.897165/post-13661337
- Erdogan (itsOVER said arguably best in the world, tho he went to emrahcinik)
- FUE (follicular extraction unit) is omst likely the only thing I’m doing. Have heard good things about FUT (where they cut a whole strip) though.
https://www.youtube.com/watch?v=t8wOzgVGYz4. Apparently FUE is overmarketed because it has a better scar position as if it matters.
- With FUE there’s minimal to no minimal shaving required (though traditionally yes, and I think it’s the cheaper and easier option), as is the case with FUT.
- In Istanbul, a hair transplant costs like $1000-$3150 (and then consider the ~$1000 2-way flight). Price per graph is maybe $0.7 or so. But some clinics don’t actually charge extra for more graphs apparently. Also, they basically do whatever you ask, so voila, just do your research.
- Shock loss: I think it’s relatively uncommon for regular tranplants, like 5-10%. It happens both in the donor and transplant area.
- One reason is due to traumatization of existing hair follicles in the area, including surrounding native areas.
- Can occur even 3 months after.
- Lng hair FUE is the real deal where donor grafts, length and all, are transplanted. Thing is, it can completey fuck you with shock loss and all the length is lost a few weeks after the operation (so it’s over). Not sure if we’ll ever get past that.W what’s the point, lol?
- Erdogan is one of the best surgeons in the world for it
- Haircafe says hair transplants last forever, and that blüdflow and scalp tension theory is bullshit, which is kind of whitepilled honestly, since that means it’s all down to genetic determinism (and donor dominance), which is more easily changeable in the grand scheme of things with drugs and whatnot.