Selegiline
links: Drugs reference: An Interview with Joseph Knoll, M.D. 10-4-2021
Selegiline
 #
#
AKA L-deprenyl. D-Deprenyl might be even better? Apparently the original maker was brought to jail.
- Irreversibly (keyword: not permanently) inhibits MAO-B, in the sense that MAO-B must be resynthesized. MAO-A is slightly inhibited in high doses (20+mg/day). The standard clinical dose is something like 10mg/day oral.
- Catecholamine release enancer
- Upregulates GDNF→VMAT2
- VP: Selegiline stabilizes VMAT2 in the correct conformation and prevents the damage caused by VMAT2 inhibitors. The dose required to do this is fixed, much lower or higher doesn’t do this and it’s unrelated to it’s MAO inhibition effect. I calculated this to be 2.2 mg buccal translated from animal studies.
- Anti-Cholinergic - so it can cause mydriasis (pupil dilation - is this the same as lsd?)
- Too much MAO-B inhibition can wreck sleep in the short term.
- Decently decreases amphetamine induced oxidative stress. Amphetamine still causes neurotoxicty through other mechanisms.
- Reversible transvestic fetishism in a man with Parkinson’s disease treated with selegiline WTF
-
Pharmacological aspects of the neuroprotective effects of irreversible MAO‑B inhibitors, selegiline and rasagiline, in Parkinson’s disease
- Increases NGF. Not sure if that’s just in strokes
- [The effect of 6-months l-deprenyl administration on pineal MAO-A and MAO-B activity and on the content of melatonin and related indoles in aged female Fisher 344N rats]
- 0.25mg/kg (HED ~2.6mg) for six months. MAO-A significantly inhibited but only after 5 hours of darkness. After 14 hours, before lights off, 5-HT, NAS, 5-HIAA and 5-HTOL levels did not differ.
-
Chronic selegiline administration transiently decreases tyrosine hydroxylase activity and mRNA in the rat nigrostriatal pathway.
- This is observed in the corpus Striatum - not substantia nigra.
- It decreased at 3/7 days but recovered by 14. And then at 21 days, TH mRNA was raised by 3x.
-
Evidence that Formulations of the Selective MAO-B Inhibitor, Selegiline, which Bypass First-Pass Metabolism, also Inhibit MAO-A in the Human Brain
- ‘Zelepar’ disintegrates and is absorbed through the buccal mucosa.
- 2.5mg/day wasn’t nothing. But in some people, the activity was actually raised.
- DAT levels were measured in 10mg group by means of cocaine binding. It’s hypothesized selegiline might inhibit it. There were only 3 subjects but yeah not a significant change.
-
Inhibition of Bupropion Metabolism by Selegiline: Mechanism-Based Inactivation of Human CYP2B6 and Characterization of Glutathione and Peptide Adducts
- CYP2B6 substrates (that which it metabolizes) also include Ketamine and Sertraline (inhibitor) and some others. Selegiline inhibits, and other inhibitors are memantine, raloxifene, curcumin, fluoxetine, fluvoxamine
-
Effects of selegiline on antioxidant systems in the nigrostriatum in rat
- 2mg/kg = 22 hed.
-
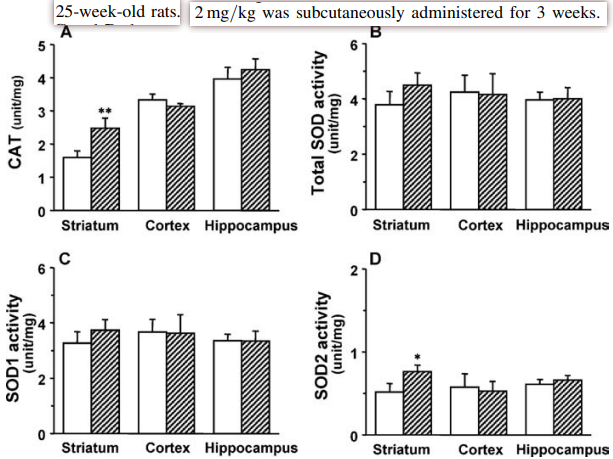 and in the 8-week old rats, yeah pretty similar results.
and in the 8-week old rats, yeah pretty similar results.
-
Effect of low‐dose treatment with selegiline on dopamine transporter (DAT) expression and amphetamine‐induced dopamine release in vivo
- 0.25mg/kg in rats = ~3mg.
| Control | 2h | 24h | 21 days |
|---|---|---|---|
| 210+-21 | 174+-30 | 324+-13 | 306+-31 |
- Can cause withtdrawal? Maybe not.
- Increasing dose lowers aggressiveness from it?
- Wtf?
Effect of low-dose treatment with selegiline on dopamine transporter (DAT) expression and amphetamine-induced dopamine release in vivo
- a reversible inhibition of dopamine uptake occurs following chronic low dose selegiline treatment in vivo which may be mediated by an increase in endogenous MAO-B substrates such as 2-phenylethylamine, rather than by the inhibitor molecule or its metabolites. Increased DAT expression appears to be a special property of the selegiline molecule, since it occurs after one low dose of selegiline, and is not seen with other inhibitors of MAO-A or MAO-B. The new DAT molecules formed following selegiline treatment appear not to be functionally active.
p-F-Deprenyl (4-Fluorodeprenyl) #
-
https://docs.google.com/document/u/0/d/1pwft7x6jn7INbogv92QU1JTHss6ru3c2dC2bxOJSfBw/mobilebasic
- Powdered p-F-Deprenyl 0.5g for $30 https://cymnootropics.com/product/p-f-deprenyl-powder-1g/ $90, from newmind
I’ve heard that p-F-deprenyl has ~60% the potency of selegiline, but is more mao-b selective. I’ve also heard it’s 2-3x stronger based on the literature newmind posted.
- If L-deprenyl metabolizes into l-amphetamine, it follows that 4-fluorodeprenyl metabolizes into 4-fluoroamphetamine and 4-fluoromethamphetamine, which are ‘serotonergic party drugs’. But they require much higher doses than regular amphetamine, almost 10x.
- The level of these metabolites is 2-4x higher than l-deprenyl.
- If the compound is racemic, then at least half of the metabolites will be of the dextro variety, so you will get high with enough, and if you do get high, it can get methhead-tier, and make you susceptible to tyramine.
Supplementation #
- lastpricepharmacy? $50 for 55x; can pay with bitcoin
- Low doses (1.25mg) everyday. To reach full MAO-B inhibition, consume 10-15mg total, and you can take it multiple times a day to quickly reach that. People take it every day for years with no negative effects.
- For ADHD, it was used at 5-10mg, and ~20mg for narcolepsy.
- Was shown to have comparable effectiveness to MPH in a trial on ADHD
- Take buccally, not orally.
- 1.25mg buccal is about equally to 10mg oral for MAO-B inihbition, and 12-14x less amphetamine metabolites.
- Oral administration is a bad idea due to the majority of your MAO being in the gut and liver. Orally, has a small amount of amphetamine metabolites, namely Levoamphetamine and Levomethamphetamine. Quite negligible, but almost completely prevented when taken bucally, which also bypasses the first-pass metabolism, eliminating risk from interactions with foods. Sirsadalot says there is tolerance. Will have to give this a look.